
Clinical Info: ACH
{kind=link}
IF at the time of assessment, all of the following are YES:
- Age 2 months +1 day to 17.99 years of age?
- Does the patient have either:
a) positive ED sepsis screen, OR
b) physician decision to treat for severe infection with poor perfusion or septic shock as evidenced by administration of parenteral antibiotics and fluid resuscitation - Patient was given, or there is intention to give IV/IO antibiotics?
- Was at least one fluid bolus administered prior to randomization, OR was the intent to give at least two boluses for abnormal perfusion?
- Has the patient received less than or equal to 40mL/kg fluid total?
AND all of the following are NO:
- Clinical suspicion of impending brain herniation?
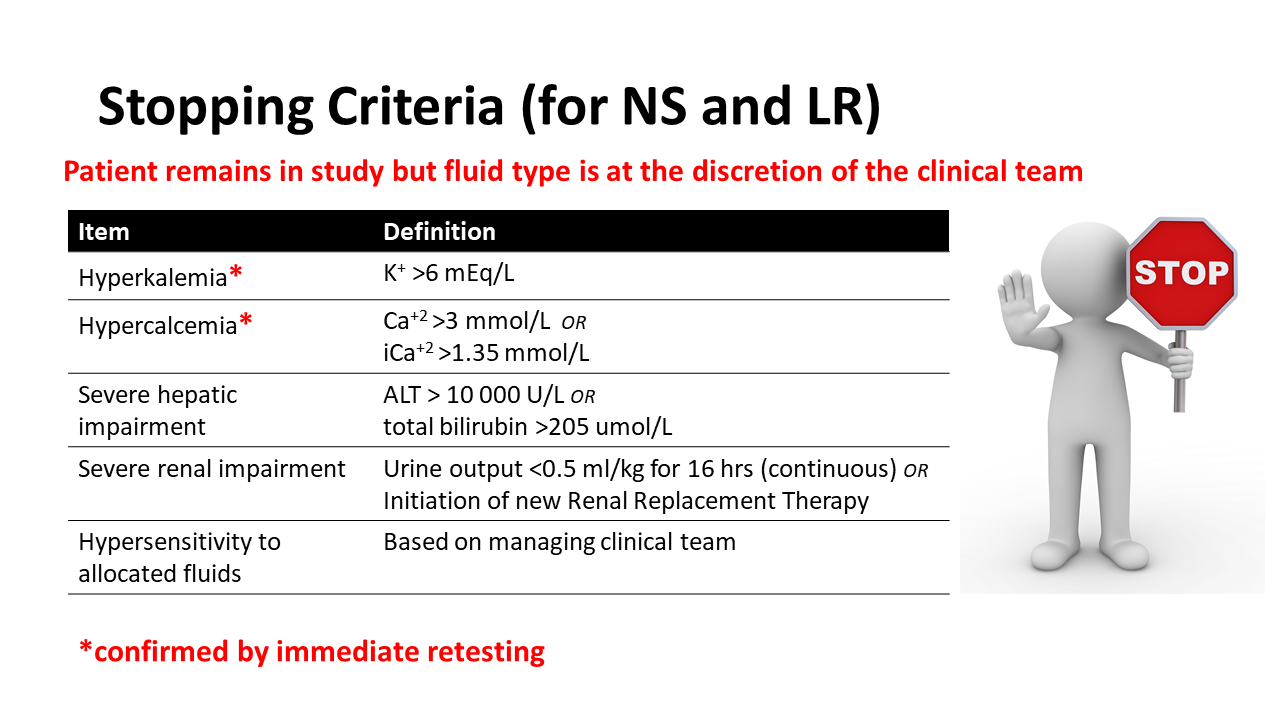
- Known hyperkalemia (>6.0mmol/L)?
- Known hypercalcemia (total calcium >3mmol/L or ionized calcium >1.35mmol/L)?
- Known acute fulminant hepatic failure, defined as plasma/serum alanine aminotransferase (ALT) >10,000 U/L or total bilirubin >205 μmol/L?
- Known history of severe hepatic impairment, defined as cirrhosis, “liver failure,” or awaiting transplant?
- Known history of severe renal impairment, defined as requiring renal replacement therapy?
- Known metabolic/mitochondrial disorder, inborn error of metabolism, or primary mineralocorticoid deficiency?
- Other concern for which the treating clinician deems it unsafe to administer either Normal Saline (NS) or Balanced Fluids (BF)?
- Known pregnancy determined by routine history disclosed by patient/caregiver?
- Known allergy to a crystalloid fluid?
then the patient is eligible for the study and you can proceed with Randomization immediately.
If the above criteria are not met – STOP, do not randomize.
Please complete the eligibility form and place it the mailbox outside the ED Research Office whether or not your patient is eligible.
Recognizing that hepatic and renal injury are a) common in septic shock, b) often improved by fluid resuscitation, and c) vary along a spectrum of mild dysfunction (common) to severe failure (uncommon), stopping criteria are defined when either an immediate unsafe condition is noted or when persistent or worsening organ injury indicates that continued LR administration may be cumulatively unsafe (e.g., potassium administration despite worsening oliguria or lactate administration despite worsening hepatic function).
{kind=link}
Dr. Graham Thompson (Principal Investigator, ED)
e-mail: graham.thompson@ahs.ca
Telephone (office): (403) 955-7295
Telephone (mobile): (403) 369-0795
Dr. Stephen Freedman (Co-Investigator, ED)
e-mail: stephen.freedman@ahs.ca
Telephone (office): (403) 955-7740
Telephone (mobile): (587) 899-8626
Dr. Suzette Cooke (Inpatient Clinical Resource)
e-mail: suzette.cooke@ahs.ca
Telephone: PHM staff can contact Dr. Cooke per standard procedures (reference internal documents)
Dr. Eli Gilad (PICU Clinical Resource)
e-mail: eli.gilad@ahs.ca
Telephone (mobile): (403) 874-6930
Beata Mickiewicz (Study Coordinator)
e-mail: beata.mickiewicz@ahs.ca
Telephone (office): (403) 955-5455
General study email (not monitored 24 hours/day): promptbolus@ahs.ca
Study team pager (Mon-Fri, 10:00-17:00): #6910